Feb 21, 2019
We read about it in the sports pages every day; the player presenting after twisting a knee, feeling a “pop” and going down in a heap. The knee is swollen, the first indication that bleeding has occurred inside the joint. Physical examination of the knee to test the ligaments leads to a suspected tear of the anterior cruciate ligament; the MRI is ordered and confirms the diagnosis.
Because of its poor blood supply and location inside the knee, the ACL has little healing potential. It’s an unfortunate reality, as they are occurring at increasing rates over the past two decades. In part, it’s because more children are playing competitive sports and doing so at a younger age while we seniors are still skiing or playing and competing all year. What are the future implications of a torn ACL? Lindsey Vonn came back after ACL surgery; so did Tiger Woods, Julian Edelman, Tom Brady and Derrick Rose to name a few. so how bad can it be? The truth is that surgery can restore knee function, but it does little to diminish the risk of arthritis 10 to 15 years down the line or less. Lindsey Vonn announced retirement five years later because of arthritis. Kids who tear their ACL today are often left with 60-year-old knees when they’re 30; and as has been recently stated, Knee Replacement is not necessarily a panacea.
Secondary damage may occur in patients who have repeated episodes of instability due to ACL injury. With chronic instability, a large majority of patients will have meniscus damage when reassessed 10 or more years after the initial injury. Similarly, the prevalence of articular cartilage lesions increases in patients who have a 10-year-old ACL deficiency. It is common to see ACL injuries combined with damage to the menisci, articular cartilage, collateral ligaments, joint capsule, or a combination of the above; the “unhappy triad,” especially in football players, soccer players, basketball players and skiers.
Certainly, modern ACL surgery means it’s no longer a career-ender, but recovery ranges still vary widely. In cases of combined injuries, surgical treatment is warranted and generally produces better outcomes. As many as half of meniscus tears may be repairable and may heal better if the repair is done in combination with the ACL reconstruction. Some athletes come back in as little as nine months, while it can take well more than a year for others. Then comes the mental battle, that is the silent war waged after tearing an ACL. Derrick Rose, we are watching you.
Recent clinical evidence suggests surgery is not your only option; interventional or cellular orthopedics may be a non-surgical alternative that uses your own cells to repair the incompletely damaged ligament. A cellular orthopedic intervention for those who meet the inclusion criteria may substitute for surgery. Those who offer the non-operative option when appropriate, use Bone Marrow or Adipose Tissue harvested from your skeleton or abdomen, process the recovered cells and growth factors with particular attention to FDA compliance, and inject the concentrate into the remaining Anterior Cruciate Ligament cumented incomplete tears with success in returning athletes to a sport.
While intervention and cellular orthopedics may have a role in a torn ACL at times, Joint Restoration, perhaps even Regeneration adjuncts at the time of an ACL repair or for the ensuing arthritis have an absolute evidence-based role. To schedule an appointment call (312) 475-1893. You may visit my web site at www.sheinkopmd.com
Tags: ACL, ACL Injury, anterior cruciate, arthritic knee, cellular orthopedic

Feb 14, 2019
Following injury or wear, limitations need not be limited to professional, college and high school athletes
Last week, my column focused on the post traumatic ravages of the National Football League season; and getting ready for next cycle of body demolition. Those who watched the championship game saw several players assisted off the field following violent trauma. Even the President announced that he would prefer his son not play football. While professional, college and high school competitive sports enjoy high profile, there are the average recreational sports and fitness enthusiasts who progressively experience a diminution of ability to participate in a sought-after activity by virtue of injury or wear and tear; be it basketball, running, cycling, skiing, hockey, fitness endeavors, volleyball, golf, soccer, sailing; so, on and so forth.
As an example, a 67-year-old man presented in my office last week after having read my column, with progressive pain in his left knee and inability to partake in his long-time recreational passion, volleyball. I completed his intake centered on the taking of his medical history, completed an orthopedic physical examination, and ordered X-rays. He brought a recent MRI study to the appointment. The physical therapist who assists me objectively documented his physical findings so we would have pretreatment measurements. Additionally, my therapeutic recommendation is always based on more than an X-Ray and MRI, but also includes the objective and reproducible Range of Joint Motion and assessment of joint stability.
After review of all the above, I administered informed consent for a Bone Marrow Concentrate intervention into his left knee as a means of postponing, perhaps avoiding a Total Knee Replacement and assisting in his return to recreational volleyball. While there are several options for intervention into the arthritic or injured joint including adipose and blood-based alternatives, I recommended Bone Marrow Concentrate for his moderately arthritic knee as a means of providing Concentrated Platelets, Concentrated Growth Factors, anti-inflammatory Cytokines, Adult Mesenchymal Stem Cells, Precursor Cells, Marrow Adipose Tissue, and Hematopoietic Cells, all consistent with FDA compliance requirements. There are mandatory Federal Drug Administration and Federal Trade Commission regulatory standards of compliance in Regenerative Medicine; patients must be cautious when choosing the minimally invasive Cellular Orthopedic option. It takes an office visit, physical assessment and review of images by a board-certified specialist in the regenerative medicine decision making process; not merely attendance at a seminar. Some patients will not meet inclusion criteria, their needs would be better served by accepted surgical norms.
At age 67, there is little chance at Cartilage Regeneration for my patient, but there is a high probability of Joint Restoration; that is increased motion, diminution of pain and the return of ability, in this patient’s case to play volleyball. He will wear an off-loader brace for six weeks, partake in physical therapy and then gradually return to his Chicago Park District three games a week routine. The patient will have reached his competitive goals through care based on the scientific evidence and outcomes documentation. As long as I introduced the subject of competitive goals, off I go to ski in Colorado next week; about a year after having undergone Cellular Orthopedic interventions to both of my arthritic hips and both of my arthritic knees. Without the biologics, not only would I be unable to ski, I would be ready for two knee replacements and two hip replacements. I should have listened to my mother and stuck to the piano and violin.
To learn more about continuing to reach your competitive goals, visit my web site www.sheinkopmd.com or call and schedule a consultation 312-475-1893).
Tags: arthritis, board-certified, Bone Marrow Concentrate, bone marrow edema, cellular orthopedics, FDA, football, Growth Factors, hematopoietic cell, joint pain, Mesenchymal Stem Cell, OA, Orthopedic Surgeon, Osteoarthritis, Physical Therapy, soccer, sports injuries, sports medicine, tear, volleyball
Jan 3, 2019
The truth about reparative medicine in orthopaedics and why it matters to you is that in the USA, millions of people suffer from orthopedic conditions and are looking for options to major surgery. At the same time, there is a segment of the population that can’t safely undergo a major joint replacement procedure. Then there are those who are highly active and are looking to keep up with their sporting activities and an unlimited life style. The older generation is living longer and very active. The younger generation is also participating in sports and playing for a longer period. The wear and tear in joints cause pain and ultimately may cause or aggravate an arthritic process. There is an option to surgery and a means of postponing, perhaps avoiding a Total Joint Replacement. While Cellular Orthopaedics (Regenerative Medicine), offers a reparative technology, it is important to recognize that all therapies in the marketplace are not equal. There are many different types of tissues: fat, bone marrow, amniotic fluid, placental tissue, cord blood, Wharton’s Jelly, and circulating blood marketed for intervention but only concentrate from your own bone marrow, concentrate and filtered platelet product from your own blood, and now micro-fractured fat from your own adipose tissue meet FDA compliance requirements.
Over the past ten years, advances in reparative medicine have resulted from science and research behind the different options. You may read about my role at www.sheinkopmd.com/published-research-articles/ to learn more. I was one of the first orthopaedic surgeons to study the effects of Micro-fractured Fat (Lipogems) in patients with Grade 4 Osteoarthritis of the knee who were en route to a Total Knee Replacement. Now that the FDA has granted clearance, many physicians are showing up with claims of offering adipose stem cells. While fat has reparative qualities and can help promote a healing environment, it is not a resource for cartilage regeneration.
As always though in the current health marketing environment, a patient must guard against misrepresentation of product, effect and outcomes. The article I published in November of 2018, is the only scholarly article of which I am aware that has true clinical adipose outcomes data. https://www.amjorthopedics.com/article/safety-and-efficacy-percutaneous-injection-lipogems-micro-fractured-adipose-tissue. Those clinics offering a type of fat technology that is processed using enzymes and manipulates the cells are doing so by failing to abide by FDA Guidance. Additionally, some providers are offering “Stem Cell Treatments” at very high costs and thus mislead the public along with the parasites, camp followers and charlatans promoting amniotic fluid, cord blood and Wharton’s jelly. Our goal is to provide the right treatment options for a patient with solutions that have strong scientific evidence behind the technology and are cleared by the FDA. I am happy to be a leader in the Evidence Based initiative.
To schedule a consultation call (312) 475-1893 You may visit my web site at www.sheinkopmd.com
Tags: adipose stem cell, fat, lipogems, micro fracture, orthopaedic, PRP, stem cell
Dec 20, 2018
How long will the benefits last?
Yesterday, an individual presented in the office on a professional matter for a scheduled business meeting and during our discussions, related that he had undergone right hip arthroscopy, eight weeks earlier. He had an antalgic (painful) gait while walking into the meeting room so I discussed the rationale for undergoing a Platelet Rich Plasma concentrate/Growth Factor Concentrate intervention when he returned to his home base. The individual elected to become my patient on the spot so I performed a physical assessment and noted asymmetrical hip motion with limitation on the right side. His pre-arthroscopic diagnosis was a torn acetabular labrum. In 45 minutes, my team had drawn his blood and prepared the concentrated injectate followed by my completing an ultrasound guided intraarticular right hip injection. Within five minutes, his inability to fully spread his legs, flex and extend his hip, and tolerate internal and external rotation had been corrected. This is not an infrequent observation following a Cellular Orthopedic intervention to the hip; yet I have no explanation for the immediate pain relief and return of joint function. He left the office with almost no discernable limp.
This past Monday, the office received this communication from a patient who began treatment with Bone Marrow Concentrate to her knees about four years ago; returning on several occasions until she reached maximum medial improvement at 18 months post intervention.
“I wanted to write to you and Dr Sheinkop to congratulate you on the published study in the Journal of Translational Medicine in which I was a participant. It is really satisfying to see that results finally in print. I want to thank you both for allowing me to participate, even though I was outside of the Chicago area.
Just to follow up, my knees have been doing really well for the past year. I enjoyed a long summer of bicycling, including regular 20-30 mile rides as well as a 40 and 50-mile ride, without significant pain. I also have been able to use the elliptical pain free and just in the past two weeks I started running on the treadmill (alternating one minute of running & walking for about 20-25 minutes on a 4% incline). I’m starting really slow -but I never thought I would be able to run relatively pain-free again”.
There is no way of predicting how soon and for how long a cellular orthopedic intervention will have an effect. Our ongoing outcomes observations for over six years may eventually help answer the question; but in the meantime, we ask our patients to return periodically so we may learn from them and intervene if needed.
To learn how you may benefit from a Cellular Orthopedic intervention schedule a consultation by calling (847)-390-7666. My web site is at www.sheinkopmd.com.
Tags: Adult Mesenchymal Stem Cells, arthritis, Bone Marrow Concentrate, cellular orthopedics, Clinical Trial. Mitchell B. Sheinkop, Growth Factors, Interventional Orthopedics, Knee Pain Relief, Mesenchymal Stem Cell, micro-fractured fat, Orthopedics, Platelet Rich Plasma, Platelet Rich Plasma concentrate/Growth Factor Concentrate, stem cells, Subchondroplasty, torn labrum

Dec 5, 2018
As interest in biologic therapies for arthritis-a needle, not a knife-continues to expand; patients increasingly are turning to the ads in newspapers or searching the Internet to gather information on this topic. While there is still a lack of scientific consensus on the use of biologics, it is most important for those seeking information not to be misled. My own analysis of resources for patients seeking on line information about biologic therapies for arthritis is that the overall quality is very poor and anything but scientific. Even worse, is a seminar, neither a reliable or credible source of scientific evidence.
Biologic therapies consist of stem cells, platelet rich plasma product and bone marrow aspirate concentrate. New research, I co-authored and that was published last month in The American Journal of Orthopedics: Safety and Efficacy of Micro-Fractured Adipose Tissue for Knee Arthritis, is indicative of the ever-evolving nature of Regenerative Medicine. Biologic therapies and their use in arthritis or musculoskeletal injury in general are an area of vast research and interest within the medical field. Understanding the information online and the misinformation provided at seminars pertaining to biologics allows me to tailor my conversation and address commonly found inaccuracies.
The use of Biologic Therapies is expected to significantly increase in the coming years as our knowledge advances on the use of such. That initiative will be led by well informed, well-educated Board Certified, and Fellowship trained specialists. Unfortunately owing to the relative lack of oversite at present, every type of charlatan, parasite and camp follower can buy an ad for a seminar or produce a web site on the internet. How then should a patient with pain and limited function from arthritis seek to postpone or avoid surgery without becoming a victim of the cord blood or amniotic fluid hoax?
- Your physician must complete a comprehensive medical history, physical examination and review of diagnostic studies.
- Explain the disease process and grade of progression,
- Discuss possible treatment options,
- Present a balanced assessment of the current scientific evidence.
Woe, while writing this Blog, I was just notified about acceptance of yet another scientific article by a peer reviewed medical journal in which I am the senior author: A Specific Protocol of Autologous Bone Marrow Concentrate and Platelet Products Versus Exercise Therapy for Symptomatic Knee Osteoarthritis; a Randomized Control Trial with 2 Year Follow-up.
Hopefully some time soon, a Biologic Arthroplasty will be possible; but until then, a Total Joint Replacement is still a necessary option for those not meeting specified inclusion criteria for biologics. To see what treatments may be possible for your arthritic generated pain call (312) 475-1893 to schedule a consultation. Visit my website www.SheinkopMD.com for additional information.
Tags: Adult Mesenchymal Stem Cells, amniotic fluid, ankle pain, arthritic pain, autologous bone marrow concentrate, biologic, biologics, cellular orthopedics, Cord blood, Hip pain, injury, joint pain, knee pain, lipogems, Osteoarthritis, PRP, regenerative medicine, rupture, shoulder pain, sports injury, stem cell, tear, tendinitis
Jul 19, 2018
The argument frequently advanced by orthopedic surgeons in response to a patient’s inquiry concerning stem cells for arthritis is that it is too early, there is not enough research, It is better to have a major surgical procedure. For those of you who have read my blog or have sought orthopedic consultation in my office, I have emphasized that my recommendations are evidence based. Each patient, for whom I have completed a cellular orthopedic intervention for arthritis, has been entered into a registry or clinical outcomes data base, IRB approved. Just as I pioneered the integration of clinical care with clinical research over 37 years as a joint replacement surgeon, so too do I now partake in the growth and development of the clinical pathways for regenerative medicine.
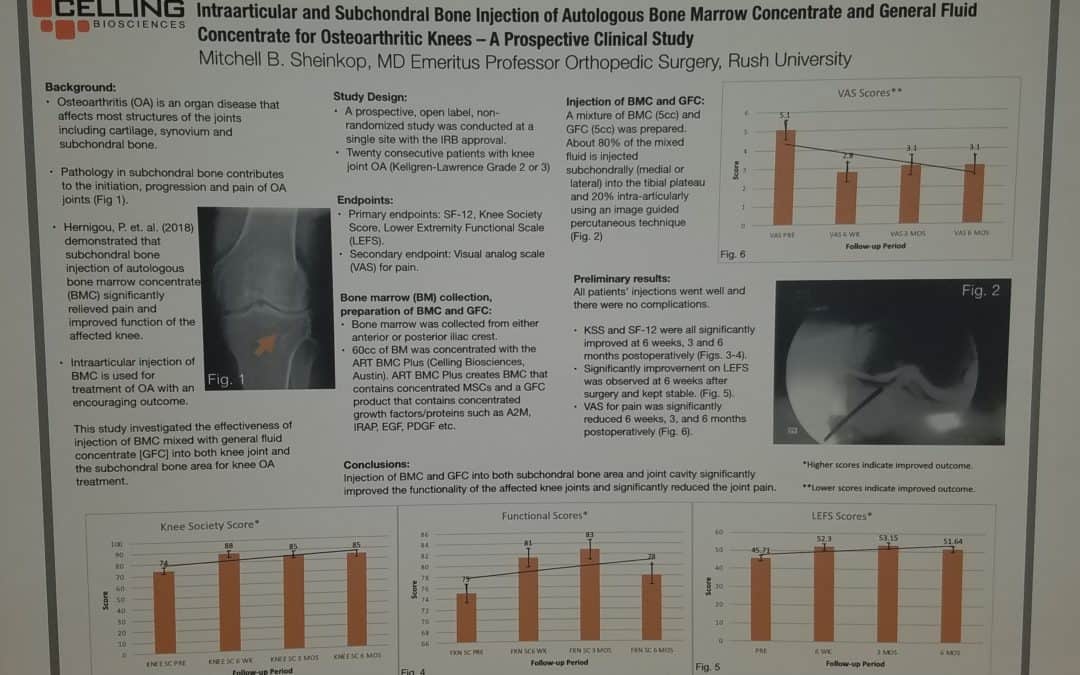
Last month, I exhibited a poster at a large regenerative medicine meeting wherein I shared my preliminary outcomes and thus educated other professionals using Intraarticular and Subchondral Bone Injection of Autologous Bone Marrow Concentrate and General Fluid Concentrate for Osteoarthritic Knees-A Prospective Clinical Study. Osteoarthritis is an organ disease that affects most structures of joints including cartilage, synovium and subchondral bone. Pathology in subchondral bone contributes to the initiation, progression and pain of Osteoarthritis. In previous European studies, the injection of autologous bone marrow concentrates into bone supporting the joint significantly relieved pain and improved function of the affected knee. The preliminary outcomes in the study that I presented via a poster exhibit, investigated the effectiveness of injections of Bone Marrow Concentrate with General Fluid Concentrate (Growth factors), into both the knee joint and the subchondral bone. The study recorded all the standard Endpoints I had previously used in joint replacement clinical outcomes trials.
Bone Marrow was collected from the pelvis and a filtration system allowed for concentration of Mesenchymal Stem Cells, Platelets, Precursor Cells and Growth factors such as A2M, IRAP, EGF, PDGF, TNF-B blocker, etc. After preparation, a mixture of Bone Marrow Concentrate and Growth factor Concentrate was injected into the bone (subchondral) and into the joint.
In the study, all patient injections went well and there were no complications. The Preliminary Results documented diminished pain and improved function. We concluded that injection of Bone Marrow Concentrate and Growth factor Concentrate into both the subchondral bone area and joint cavity significantly improved function of the affected knee joints and significantly reduced joint pain. While there are many stem cell providers to be found because of their marketing, choose the center of excellence in Cellular Orthopedics that is evidence based.
Call to schedule a scientific based consultation from an orthopedic surgeon 1 (312) 475-1893.
You may access my web site at www.SheinkopMD.com.
Tags: avascular necrosis, bone lession, bone marrow, Cartilage, cellular orthopedics, clinical study, Growth Factors, IRAP, joint pain, joint replacement, knee pain, knee replacement, meniscus tear, Osteoarthritis, platelets, PRP, regenerative medicine, sports medicine, stem cells, subchondral bone